The pressure to act is structural. The AAMC projects a U.S. shortage of up to 86,000 physicians by 2036, while HRSA's model puts that figure at 141,160 by 2038. Meanwhile, 21.7% of U.S. adults delayed or skipped care due to nonfinancial barriers — no available appointments, no reachable provider. Conversational AI doesn't solve physician shortages. But it does address the access gap between when patients need care and when a physician is available to provide it.
This article covers what the 2025–2026 evidence actually shows, what "clinical readiness" requires beyond benchmark scores, where deployment is working today, and what infrastructure is needed to make it real.
Key Takeaways
- Landmark studies show conversational medical AI can match or exceed physician performance on specific clinical dialogue tasks under supervised conditions
- "Clinical readiness" in 2026 means structured human-AI collaboration — physician oversight is non-negotiable, not optional
- Patient acceptance is higher than expected, with documented improvements in satisfaction and clarity vs. standard care
- Safe deployment requires clinical validation, HIPAA-compliant infrastructure, and a staged rollout — a capable language model alone is not enough
- Without the right cloud foundation, organizations cannot deploy these systems securely or at scale
From Research to Reality: What the Evidence Shows
The AMIE Study: A Clinical Milestone
Google's AMIE study, published in Nature in 2025, ran a randomized, double-blind OSCE-style evaluation across 159 case scenarios. The LLM-based system outperformed primary care physicians on 30 of 32 specialist-rated axes and 25 of 26 patient-actor axes.
The key finding: AMIE's diagnostic advantage came not from gathering more information, but from interpreting the same information more accurately into a complete differential diagnosis. This suggests AI reasoning and human clinical judgment are complementary — AI can process and synthesize conversational data at scale; physicians bring contextual judgment that no model fully replicates.
The study used text-only interfaces in simulated settings, and synchronous text chat is unfamiliar in routine practice. These aren't reasons to dismiss the findings — but they define the limits of what the data actually proves.
Mo: The First Large-Scale Real-World RCT
Where AMIE tested a controlled simulation, Mo tested the real thing. Alan Health Insurance's deployment, documented in a preprint on arXiv, is the first large-scale RCT of a physician-supervised conversational agent in an actual clinical setting. Across 926 cases, 298 patients completed AI-led conversations.
Key results:
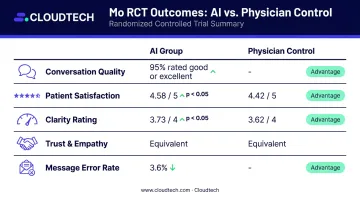
- 95% of conversations rated "good" or "excellent" by supervising GPs
- No conversation was deemed dangerous overall (one contained potentially dangerous inaccuracies)
- 3.6% of individual messages were rated poor; three were hidden by physicians
- Patient satisfaction: 4.58/5 vs. 4.42/5 for the control group (p < 0.05)
- Clarity ratings: 3.73/4 vs. 3.62/4 (p < 0.05)
- Trust and empathy scores were statistically equivalent between AI and physician control
The opt-in rate tells its own story: 81% of eligible patients chose to engage with the AI system — a figure that exceeds prior benchmarks for patient acceptance of clinical AI.
AI's near-instantaneous response time (median 0.2 minutes vs. 4.8 minutes for physicians) produced faster patient responses too — median 1.1 vs. 2.8 minutes. More fluid exchanges mean more complete clinical information, which means better triage and earlier help-seeking.
Limitations across both studies: simulated or short-duration environments, GP-only coverage, small samples for rare cases, and — in Mo's case — an approximate 20% survey response rate. Each gap points to a specific question that the next generation of trials needs to answer.
What "Clinical-Grade" Actually Means in 2026
The phrase gets used loosely. In practice, clinical readiness requires simultaneous performance across all of the following dimensions:
- History-taking accuracy
- Diagnostic reasoning quality
- Communication clarity and tone
- Demonstrated empathy
- Patient safety under edge-case conditions
A system that excels on one axis while failing another doesn't qualify.
The Physician Oversight Model
The Mo deployment provides the clearest available template for what effective oversight looks like in practice:
- Real-time message review within 15 minutes by a supervising GP
- Authority to intervene at any point — stop the agent, edit a message, or override its direction
- Mandatory physician check-in at the end of every AI-led conversation
This isn't a backup system. It's a structural component of the deployment. Remove physician oversight and the safety profile changes entirely.
Staged Rollout as the Industry Standard
Alan's phased approach is worth examining as a model:
- Internal employees — lowest-risk population, highest organizational control
- Small member cohort under close physician supervision
- Broader rollout with all service physicians trained and monitoring
Each phase generates data that informs the next. Edge cases surface before scale amplifies them. This approach isn't just cautious — it's what distinguishes responsible clinical AI introduction from a product launch.
What Clinical-Grade Does NOT Mean
- Not autonomous diagnosis
- Not a replacement for specialist consultations
- Not a system that operates without continuous monitoring after go-live
- Not a solution that works without a HIPAA-compliant infrastructure beneath it
Organizations that treat conversational AI as a cost-cutting shortcut will find themselves exposed on two fronts: patient safety incidents and regulatory enforcement under HIPAA and FDA Software as a Medical Device (SaMD) guidance, both of which apply directly to AI systems making or influencing clinical decisions.
Where Conversational Medical AI Is Making an Impact Today
Patient Engagement and Chronic Disease Management
Between care episodes, patients with chronic conditions — hypertension, diabetes, COPD — face a gap. They have questions about medications, notice symptom changes, and often wait days for a callback. Conversational AI is filling that space.
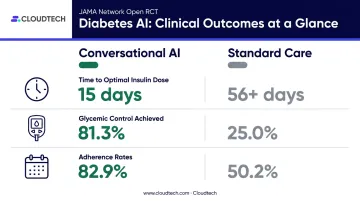
A voice-based conversational AI trial in diabetes management, published in JAMA Network Open (2023), found striking results in a 32-person RCT:
- Median time to optimal basal-insulin dose: 15 days vs. more than 56 days
- Glycemic control achieved: 81.3% vs. 25.0%
- Adherence rates: 82.9% vs. 50.2%
The sample is small and the study short. But the direction is consistent with what Mo demonstrated — that faster, more accessible information exchange produces measurably better patient behavior.
Clinical Decision Support and Workflow Efficiency
The volume of medical literature makes manual evidence review increasingly impractical. Conversational AI integrated into clinical decision support tools lets clinicians ask specific, contextual questions — drug safety in pregnancy, dosing for renal impairment, contraindication flags — without leaving their workflow to search databases.
That said, performance varies dramatically by use case. A 2026 Nature Medicine synthetic stress test found that ChatGPT Health failed to escalate 51.6% of emergencies and overtriaged 64.8% of non-urgent cases in a vignette-based evaluation. Validation against the specific clinical task matters far more than general benchmark scores.
On the administrative side, conversational AI is handling tasks that consume significant staff time:
- Routing patients to the right care pathway
- Scheduling and rescheduling appointments
- Answering routine queries (hours, refill requests, pre-visit instructions)
This frees clinical staff to focus on complex cases where human judgment is genuinely needed.
Safety, Compliance, and the Physician Oversight Model
Regulatory Requirements
For U.S. healthcare organizations, the baseline requirements include:
- HIPAA: Any AI vendor handling electronic Protected Health Information (ePHI) must sign a Business Associate Agreement (BAA) with the covered entity. Encryption is an addressable specification — implement it when reasonable and appropriate, or document an equivalent measure
- FDA: Not every conversational tool qualifies as a Software as a Medical Device (SaMD). Applicability depends on intended use and whether the system meets device software function criteria
- EU AI Act: Entered into force August 1, 2024, with general application from August 2, 2026. Article 2 reaches non-EU providers whose output is used in the EU — U.S. healthcare systems serving international populations should take note
Layered Safety Architecture
Responsible deployments use multiple protection layers:
- Scope limitations — AI is automatically inactivated for out-of-scope queries (psychological emergencies, specialist-only conditions)
- Explicit transparency — patients know they are interacting with an AI, not a physician
- Real-time physician intervention — not periodic review, but active monitoring with immediate override capability

Bias: A Non-Negotiable Testing Requirement
AMIE's ablation testing found reduced differential-diagnosis performance for patients with low English literacy. This is a direct demonstration of how bias in training data translates directly into clinical performance gaps — and given existing health inequities, amplifies them.
Diverse patient testing and red-teaming before deployment are requirements, not recommendations.
Continuous Post-Deployment Monitoring
Pre-deployment validation is necessary but not sufficient. The FDA/Health Canada/MHRA Good Machine Learning Practice principles explicitly call for deployed-model monitoring and management of retraining risks. Clinical knowledge evolves. Edge cases that don't appear in a three-week study surface at scale over months.
Two commitments separate responsible deployments from reckless ones:
- Ongoing monitoring — tracking model performance against real-world outcomes, not just pre-launch benchmarks
- Retraining governance — defined protocols for when and how models are updated as clinical knowledge changes
Organizations that treat go-live as the finish line carry risk they may not recognize until a patient is harmed.
Cloud Infrastructure: The Foundation Behind Clinical AI Deployment
Conversational medical AI doesn't run on goodwill and a capable model. It runs on infrastructure. Multi-agent systems like Mo require real-time orchestration across multiple models, compliant data storage, low-latency chat interfaces, and HIPAA-eligible compute environments.
What the Infrastructure Stack Requires
| Requirement | Why It Matters |
|---|---|
| HIPAA-eligible cloud services | PHI handling requires a BAA and compliant configuration |
| End-to-end encryption | Data at rest and in transit must be protected |
| Region-specific data residency | HIPAA and EU AI Act both impose geographic constraints |
| Horizontal scalability | Patient volume spikes can't degrade response times |
| Audit logging | Physician review workflows require tamper-evident records |
AWS officially lists Amazon Bedrock, AWS HealthLake, EC2, and S3 as HIPAA-eligible services — but eligibility is not automatic compliance. PHI workloads require a signed AWS BAA and HIPAA-consistent customer configuration.
A 2025 KLAS survey found that nearly 40% of healthcare organizations still kept the majority of their infrastructure on premises, with cloud cost and healthcare-specific expertise cited as top concerns. Bridging that gap requires both the right architecture and the expertise to configure it compliantly from day one.
How Cloudtech Supports Healthcare Organizations
Cloudtech, an AWS Advanced Tier Partner based in New York, helps healthcare SMBs architect the compliant cloud foundations that clinical AI systems require. Their work with Klamath Health Partnership shows what this looks like in practice:
- HIPAA-compliant data lake on Amazon S3
- Multi-account governance via AWS Organizations and Control Tower
- Centralized audit logging through AWS CloudTrail
- PHI encryption using AWS KMS
- Automated sensitive data discovery with Security Hub, GuardDuty, and Amazon Macie
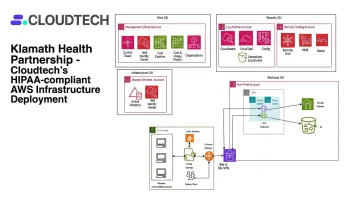
The result for Klamath: a 77% year-over-year reduction in infrastructure costs, alongside a fully audit-ready, HIPAA-compliant environment.
For healthcare organizations building toward conversational AI deployment, Cloudtech also offers Clinical Document AI using Amazon Textract and Comprehend Medical. The service automates extraction of structured data from clinical PDFs, faxes, and charts — at cents per page versus $8–15 per chart manually. That structured data layer is what gives conversational AI systems accurate, accessible clinical context to work from.
Frequently Asked Questions
Is conversational medical AI ready to replace doctors?
No. In 2026, every evidence-backed deployment studied operates under physician oversight as a structural requirement, not a safeguard that might be phased out. The clinical task is augmentation — handling volume, improving access, and extending the reach of physician judgment.
What clinical tasks can conversational AI handle safely today?
Validated use cases include routine medical Q&A, history-taking support, chronic disease check-ins, patient triage and routing, and clinical decision support queries. Complex diagnosis, specialist consultations, and psychological emergencies remain physician-led.
How accurate is medical conversational AI compared to physicians?
Results vary by context, but leading studies are encouraging: the AMIE system outperformed primary care physicians on 30 of 32 specialist-rated axes, and 95% of AI-led conversations in the Mo trial earned "good" or "excellent" ratings from supervising GPs. Clinical context, specialty, and oversight quality all affect real-world accuracy.
What are the biggest risks of deploying conversational AI in healthcare?
The primary risks are diagnostic errors in rare or complex cases, AI bias against underrepresented patient populations, over-reliance without adequate physician oversight, and data privacy breaches if the underlying infrastructure is not HIPAA-compliant.
What does it take for a healthcare organization to deploy conversational AI?
A successful deployment requires:
- Clinical validation framework and physician oversight protocols
- HIPAA-compliant cloud infrastructure with documented compliance
- Patient consent mechanisms and a staged rollout plan
- Continuous post-deployment monitoring
This is a cross-functional initiative, not an IT project.
How should healthcare organizations evaluate a conversational AI vendor?
Prioritize vendors who supply real-world performance data from clinical deployments, disclose training data sources and model limitations, show documented HIPAA compliance and AI regulatory alignment, and build physician oversight into the product architecture from day one.