The numbers bear this out. According to ASTP/ONC, 71% of U.S. non-federal acute-care hospitals used predictive AI integrated with their EHRs in 2024 — up from 66% in 2023. Yet among independent hospitals, that figure drops to just 37%, compared to 86% for system-affiliated institutions. The gap isn't just about adoption. It's about what happens after deployment.
Most healthcare organizations — particularly community health systems and specialty practices — are deploying AI tools without the governance infrastructure to validate, monitor, or course-correct them. That's where the real risk lives.
This article makes the case that AI governance isn't a constraint on innovation. It's the mechanism that allows AI to scale responsibly, reach more patients, and generate sustainable returns for your organization.
Key Takeaways
- AI governance covers tool selection, validation, deployment, and monitoring — skipping it turns scaling into compounding clinical and legal risk
- Racial bias, poor vendor performance, and clinician over-reliance are documented failure modes, not hypothetical ones
- A seven-domain governance framework works for organizations of any size, not only large academic health systems
- HIPAA-compliant cloud infrastructure (audit logging, monitoring, access controls) is the technical backbone that makes governance real
- Smaller organizations close the governance gap by outsourcing infrastructure while keeping clinical oversight in-house
Why Governance Enables — Rather Than Slows — Healthcare AI Scaling
The "governance slows us down" concern is understandable. Committees, documentation requirements, and review cycles feel like friction when clinical leaders are eager to deploy tools that promise faster diagnoses or reduced administrative burden. The evidence, though, points in a different direction.
The Regulatory Gap Is Real, and It Falls on You
Unlike pharmaceuticals or medical devices, clinical AI currently operates in a space of limited federal oversight. Health systems bear primary responsibility for validating, monitoring, and taking accountability for the AI tools they deploy.
The FDA has issued guidance on Predetermined Change Control Plans for AI-enabled device software, but most diagnostic support and administrative AI tools fall outside formal device regulation entirely. That means your governance framework, or the absence of one, is the primary safety net for your patients.
Unmonitored AI Causes Measurable Harm
The consequences of ungoverned AI aren't abstract. Two landmark studies show what happens when oversight is missing:
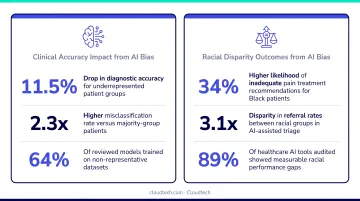
- Algorithmic bias in population health: Obermeyer et al. (Science) found a widely used algorithm used healthcare cost as a proxy for medical need, systematically assigning Black patients lower risk scores than White patients with equivalent illness burden. Fixing the proxy variable would have increased the share of Black patients receiving additional care from 17.7% to 46.5%. The bias wasn't in the model's code — it was a target variable choice made during problem formulation, exactly what a governance framework catches before deployment.
- Clinician accuracy degradation: A 2023 randomized study in JAMA found that clinician diagnostic accuracy decreased by 11.3% when systematically biased AI predictions were shown alongside explanations. Governance has to extend beyond model validation to how clinicians interact with AI output.
Governed AI Moves Faster at Scale
These risks don't disappear on their own — they get managed or they compound. That's precisely where structured governance shifts from compliance overhead to competitive infrastructure.
Organizations with mature governance frameworks don't spend months debating each new AI tool from scratch. They apply pre-defined evaluation criteria, test against consistent standards, and generate the documentation needed to justify expansion to new departments. That process is faster than ad hoc review — and far less likely to result in a deployment that gets pulled six months later when performance problems surface.
The Core Pillars of a Healthcare AI Governance Framework
A 2026 systematic review in npj Digital Medicine analyzed 35 health AI implementation frameworks published between 2019 and 2024 and identified seven governance domains that recur across leading models. These domains are not sequential steps: they function as an interconnected system, and weakness in any one area undermines the others.
| Domain | What It Addresses |
|---|---|
| Organizational Structure | Oversight body, decision rights, risk escalation |
| Problem Formulation | Use case prioritization, target variable selection |
| Vendor/Algorithm Evaluation | Third-party tool assessment, transparency requirements |
| Algorithm Development | Training data standards, data quality controls |
| Model Validation & Fairness Testing | Independent validation, demographic subgroup analysis |
| Deployment & Workflow Integration | Shadow deployments, clinician training, alert fatigue |
| Continuous Monitoring | Post-deployment performance tracking, bias drift audits |

Organizational Structure and Oversight
An effective AI governance body is multidisciplinary by design. Core members should include:
- Clinical leadership to flag workflow impact before tools go live
- IT and data science to assess technical feasibility and integration
- Legal and compliance to address liability and regulatory exposure
- Bioethics and patient representation to ensure equitable outcomes
Without clinical voices, governance bodies approve tools that create problems on the floor. Without legal input, liability exposure goes unaddressed.
Smaller organizations don't need a standalone AI governance office on day one. A lightweight committee integrated into an existing quality improvement or clinical informatics structure is a legitimate starting point, provided it has defined decision rights and a clear escalation pathway.
Data Quality, Validation, and Bias Prevention
Training data must reflect the patient population the model will serve. Validation on independent datasets (not the same data used to train the model) is a hard requirement: models validated only on their own training data routinely overstate real-world performance. Fairness testing across demographic subgroups catches the kind of proxy-variable bias that the Obermeyer study documented.
One often underestimated risk is dataset shift: over time, your real-world patient population diverges from the training data, and model performance degrades without warning. Validation requires ongoing reassessment with defined triggers, not a single sign-off at deployment.
Deployment, Integration, and User Training
Shadow deployments (running AI alongside existing workflows without acting on its outputs) allow organizations to evaluate real-world performance before committing to full integration. This catches problems that internal testing misses.
User training must go beyond teaching clinicians how to use the tool. It needs to address:
- The model's known limitations and failure modes
- Appropriate scope of use (what the tool should not be used for)
- How to recognize and report suspicious outputs
- The risk of automation bias — over-trusting AI recommendations without independent clinical judgment
Continuous Monitoring and Post-Deployment Oversight
This is the most under-resourced governance domain in most health systems. A 2021 external validation of the Epic Sepsis Model (one of the most widely deployed proprietary clinical AI tools in the U.S.) reported an AUC of 0.63, sensitivity of 33%, and a positive predictive value of just 12% at the evaluated threshold. The model had been broadly implemented based on vendor claims without systematic local validation.
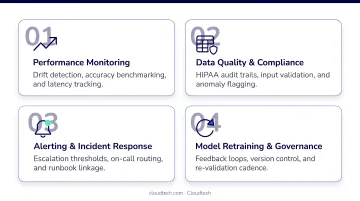
Post-deployment monitoring requires:
- Real-time performance dashboards with defined thresholds for intervention
- Incident reporting channels accessible to frontline clinicians
- Regular bias audits across demographic subgroups
- Defined protocols for model retraining or decommissioning
For adaptive AI models that update based on new data, monitoring requirements are even more stringent. The FDA's 2025 guidance on Predetermined Change Control Plans addresses how algorithm modifications should be managed as a regulated process.
Assessing Your Organization's AI Governance Maturity
The HAIRA Maturity Model
The Healthcare AI Governance Readiness Assessment (HAIRA), published in npj Digital Medicine, provides a five-level framework that spans all seven governance domains — from Level 1 (ad hoc, no formal governance body) to Level 5 (leading academic health system with full internal validation capabilities and proactive risk management).
What early maturity looks like (Levels 1–2):
Relying on vendor certifications as the primary validation mechanism
No named governance body with defined decision rights
Basic acceptance testing at deployment, no post-deployment monitoring plan
Transitioning to: documented evaluation procedures, a cross-disciplinary oversight committee, standardized testing checklists
What mid-to-advanced maturity looks like (Levels 3–4):
- Full internal validation capabilities for externally sourced AI tools
- Dedicated clinical informatics or data science resources
- Change management processes for model updates
- Proactive bias monitoring across demographic subgroups
One critical principle from the HAIRA framework: an organization's governance maturity is determined by its lowest-scoring domain, not its strongest. An organization with excellent vendor evaluation processes but no post-deployment monitoring is not a Level 3 organization.
A Practical Self-Assessment
Four questions to determine your current governance level:
- Do you have a named governance body with defined decision rights over AI tool selection, deployment, and decommissioning?
- Is there a live monitoring system with an incident reporting pathway accessible to frontline clinical staff?
- Do you conduct bias and subgroup fairness testing before deployment — not just overall accuracy testing?
- Do you have a documented process for model retraining or decommissioning when performance thresholds are breached?
If you answered "no" to two or more of these, your organization is operating at Levels 1–2. That gap is common — and it points directly to a resource problem, not just a process one.
Closing the Resource Gap
Most published governance frameworks were designed with large academic health systems in mind. The issue: ASTP/ONC data shows independent hospitals — the organizations with the fewest internal AI resources — are also the ones with the lowest AI adoption and the fewest formal governance structures.
Organizations without in-house data science teams can still implement structured governance by separating technical and clinical responsibilities. Clinical oversight, use case prioritization, and ethics review stay internal. The infrastructure layer can be outsourced:
- HIPAA-compliant cloud architecture
- Model monitoring and drift detection
- Audit logging and access controls
- Data pipeline management
An experienced AWS partner handles this layer so clinical and compliance teams can focus on the oversight work only they can do.
Cloudtech works with smaller healthcare organizations to build exactly this infrastructure on AWS — configuring compliant environments, standing up monitoring pipelines, and handling the technical setup that most independent hospitals lack the internal capacity to manage.
The Cloud Infrastructure That Makes Governance Scalable
Governance is not just a policy document. Without technical infrastructure to support it, policies don't translate into operational reality. For healthcare organizations scaling AI, the cloud layer is where governance becomes functional.
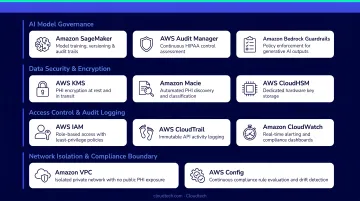
A governance-ready AWS environment for healthcare typically includes:
- HIPAA-compliant data storage via AWS HealthLake, supporting FHIR-standard health data with appropriate access controls
- Audit logging through AWS CloudTrail, creating an immutable record of API activity and data access for compliance review
- **Role-based access controls for PHI** managed through AWS IAM Identity Center and AWS KMS encryption
- Real-time monitoring via Amazon CloudWatch, with alerting thresholds for performance anomalies
- Data drift detection through Amazon SageMaker Model Monitor, which uses defined rules to flag when incoming data diverges from training distributions
- Centralized data governance through AWS Lake Formation, with fine-grained access controls for S3 data and analytics pipelines
For smaller healthcare organizations, the practical advantage of a cloud-native approach is that these capabilities don't require an internal infrastructure team to build and maintain.
Cloudtech's AWS-certified team has built HIPAA-compliant cloud environments that incorporate these governance-relevant components for healthcare clients — audit logging, access controls, and monitoring infrastructure included as standard deliverables.
The architecture Cloudtech established for Klamath Health Partnership, for example, achieved a 77% year-over-year reduction in infrastructure costs while establishing a secure, compliant data lake foundation.
Governance Mistakes Healthcare Organizations Must Avoid
Mistake 1: Treating governance as a one-time approval
AI governance is a lifecycle function, not a deployment checkbox. Patient populations change, workflows evolve, and model performance drifts. Organizations that review AI tools at launch and never reassess are accumulating risk they can't see.
The Epic Sepsis Model is a direct illustration: broad deployment without ongoing local monitoring produced clinical AI making recommendations with a PPV of 12%.
Mistake 2: Excluding clinicians from governance decisions
Governance structures dominated by IT and data science without direct clinical input miss workflow integration problems, set misaligned use case priorities, and fail to build the frontline trust needed for genuine adoption.
ASTP/ONC data shows 56% of hospitals use clinical decision support committees in AI evaluation. Nearly half don't — and that's a structural gap with real consequences.
Mistake 3: Over-relying on vendor claims
Vendor benchmarks and internal certifications are not a substitute for independent validation against your specific patient population and clinical context. Before deployment, request transparency into:
- Training data composition and known limitations
- Validation methodology and datasets used
- Subgroup performance across demographic groups
- Known failure modes and edge cases
Then validate those claims independently. If a vendor won't provide that information, treat it as a governance disqualifier.
Frequently Asked Questions
What is AI governance in healthcare and why does it matter?
AI governance is the structured set of processes, oversight bodies, and policies that guide how AI tools are selected, validated, deployed, and monitored in clinical settings. Without it, organizations face compounding risks to patient safety, regulatory compliance, and clinical effectiveness — with no systematic way to detect problems before they cause harm.
What are the key pillars of a healthcare AI governance framework?
Seven core domains form the framework: organizational oversight, use case prioritization, vendor evaluation, data quality, model validation, deployment integration, and post-deployment monitoring. Each domain feeds into the others — gaps in one will surface as failures in another.
How can smaller healthcare organizations implement AI governance without a large internal AI team?
A tiered approach allows organizations to start with a lightweight governance committee embedded in existing quality or IT structures. Technical components — cloud infrastructure, monitoring, audit logging — can be outsourced to an experienced AWS partner, while clinical oversight and ethics review remain internal. Governance doesn't require a dedicated AI team to be functional.
What role does cloud infrastructure play in scaling healthcare AI governance?
HIPAA-compliant cloud infrastructure provides the technical backbone for governance — including audit logging, role-based access controls for PHI, real-time monitoring dashboards, and drift detection for deployed models. Without this infrastructure, governance policies remain aspirational rather than operationally enforced.
How should healthcare organizations monitor AI performance after deployment?
Effective post-deployment monitoring combines real-time performance dashboards, bias audits across demographic subgroups, and incident reporting channels that frontline clinical staff can actually access. Critically, thresholds for retraining or decommissioning a model should be set before go-live — waiting for a problem to surface is too late.
What is an AI governance maturity model and how does it apply to our organization?
A maturity model like HAIRA scores your organization across all seven governance domains on a scale from ad hoc (Level 1) to optimized (Level 5). It helps identify which domains are dragging down overall maturity so you can set advancement targets that match your actual resources and structure.