Introduction
In May 2023, the National Eating Disorders Association disabled its Tessa chatbot after users reported receiving advice to lose 1–2 pounds per week and follow a 500–1,000 calorie daily deficit. The chatbot was designed for eating disorder prevention. What went wrong? According to NPR's reporting, Tessa was originally rule-based — but a vendor added generative AI capabilities without NEDA's knowledge, turning a controlled tool into an unpredictable one.
Tessa wasn't an isolated failure. The 2024 HIMSS Healthcare Cybersecurity Survey found that **42% of healthcare organizations lacked formal AI approval processes**, and 11% weren't even sure whether they had one.
Healthcare chatbots sit at a different risk level than other software. They interact directly with patients around sensitive health concerns — which means a guardrail failure isn't just a product bug. It's a patient safety event with potential HIPAA, legal, and reputational consequences.
This article covers the essential guardrail strategies healthcare organizations need to deploy AI chatbots safely: from content filters and clinical escalation protocols to vendor oversight and compliance architecture.
Key Takeaways
- Healthcare chatbots require guardrails across three phases: pre-deployment testing, real-time conversation controls, and post-deployment monitoring
- The Tessa incident shows how vendor-introduced changes can silently breach scope boundaries — undetected by the deploying organization
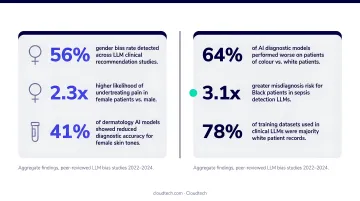
- Bias in medical AI outputs is pervasive — a 2025 systematic review found gender disparities in 93.7% of studies and racial/ethnic bias in 90.9%
- State-level laws in California, Illinois, and Texas now impose specific restrictions on AI behavior in healthcare contexts
- One-time guardrail setup — rather than continuous discipline — is the most common and most dangerous mistake
What AI Guardrails Actually Mean in Healthcare
AI guardrails in healthcare are the technical, operational, and policy controls that define what a chatbot can and cannot do. They govern scope, response accuracy, escalation behavior, and data handling.
Without them, a chatbot might answer a question it shouldn't, miss a patient in crisis, or surface information it has no business providing.
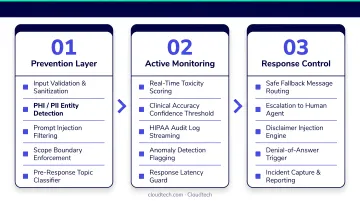
Guardrail effectiveness depends on three phases working together:
- Pre-deployment — testing and validation before any patient sees the system
- Real-time — controls that govern every conversation as it happens
- Post-deployment — monitoring that catches drift, failure, and new risk patterns over time
Failing in any one phase creates patient risk, regardless of how well the other two are handled. The Tessa case is a clean example: pre-deployment guardrails existed, but there was no real-time or post-deployment mechanism to detect that the underlying system had fundamentally changed.
The Non-Negotiable Baseline
Every healthcare chatbot, regardless of use case, must meet a minimum standard:
- Patients must know they are not speaking with a clinician (transparent AI identity)
- The system must recognize what it cannot answer and refuse clearly (defined scope limits)
- A documented route to a human must exist and must actually work (escalation path)
Accidental misuse (a confused patient asking the wrong question) is only part of the risk. Guardrails must also defend against deliberate manipulation. Common adversarial threats include:
- Prompt injection attempts designed to override system instructions
- Social engineering to extract protected health information (PHI)
- Persistent pressure to push the bot into clinical territory
Single-point controls fail against these inputs. Layered defenses are required.
Pre-Deployment Guardrails
Validate Against Real Patient Language, Not Just Training Data
A model that performs well on curated training data can fail badly on actual patient interactions. Patients don't use clinical language. They abbreviate, they're vague, they describe symptoms in ways that don't map cleanly to any training set. Pre-deployment validation must expose the model to real-world messiness before go-live — not just benchmark it against clean data.
Testing must cover two interaction types:
- Single-turn: basic FAQs, appointment scheduling, hours and location queries
- Multi-turn: rescheduling flows, medication refill intake, billing disputes that span multiple exchanges
Historical patient interaction data, replayed against updated agent logic, is one of the most effective ways to catch unintended regressions before they reach patients.
Bias Testing Is Not Optional
A 2025 systematic review of medical LLMs found gender disparities in 15 of 16 studies (93.7%) and racial or ethnic bias in 10 of 11 studies (90.9%). One evaluated model predicted a 56.54% death rate for White patients and 62.25% for Black patients on identical inputs. These are not hypothetical risks.
Pre-deployment bias testing should:
- Validate outputs across demographic subgroups with documented results
- Test for diagnostic, triage, and recommendation disparities
- Flag differential performance before the system touches a single patient
The ONC's HTI-1 Final Rule (effective March 11, 2024) established transparency requirements for predictive decision support interventions in certified health IT — covering fairness, validity, safety, and risk management. While not a direct rule for all patient-facing chatbots, it sets a benchmark that any healthcare organization deploying these systems should apply.
AWS Tools for Pre-Deployment Control
Addressing bias and scope risks requires the right tooling in place from day one. Amazon Bedrock Guardrails — available on HIPAA-eligible AWS infrastructure — provides configurable content filters, denied topic lists, sensitive information filters, and contextual grounding checks. These can enforce scope boundaries before deployment. Cloudtech, an AWS Advanced Tier Partner, helps healthcare SMBs configure these guardrails to meet HIPAA standards — from content filter policies to grounding checks — without the overhead typically associated with enterprise implementations.
Real-Time Operational Guardrails
Response Supervision Before Delivery
Before any message reaches a patient, the system should verify:
- Is the response grounded in approved information sources?
- Is it relevant to what the patient actually asked?
- Does it hallucinate details, invent capabilities, or make promises the system cannot keep?
"Plausible" is not "correct" in a clinical context. A chatbot that sounds confident while fabricating medication information is more dangerous than one that simply says it doesn't know. That hallucination risk is exactly what Amazon Bedrock's contextual grounding check addresses — detecting fabricated responses when source context and user query are both provided, giving you a meaningful control at the output layer.
Escalation as a Core Feature, Not a Fallback
Escalation triggers should be configured liberally, not minimally. The conditions that always route to a human include:
- Patient expressions of emotional distress or crisis language
- Any request for clinical advice, symptom interpretation, or medication guidance
- Sensitive billing disputes or insurance questions
- Repeated interaction failures within the same session
- Any explicit request to speak with a person
A clean escalation handoff passes the full conversation summary and collected context to the receiving agent. Patients should not have to repeat themselves. Forcing a patient to restart from scratch is a patient experience failure — and for someone in crisis, it can directly delay care.

Speed vs. Safety Tradeoffs
Some guardrail checks can run in parallel with response generation to minimize latency. Others must gate the response before delivery. A guardrail system that slows the chatbot to the point where patients abandon the interaction is itself a patient safety risk.
Design the check order with that tension in mind:
- Run non-blocking checks (input classification, topic filtering) in parallel with generation
- Gate only high-stakes checks (hallucination detection, crisis language screening) before delivery
- Test under realistic patient load before go-live — latency issues rarely surface in low-volume staging environments
Data, Privacy, and Compliance Guardrails
HIPAA and the Proposed Security Rule Update
HHS issued a Notice of Proposed Rulemaking in January 2025 that would strengthen the HIPAA Security Rule. If finalized, it would add:
- Technology asset inventories and stronger risk analyses
- Multi-factor authentication and encryption requirements
- Vulnerability scanning every six months
- Annual penetration testing
This rule is proposed, not yet final. Healthcare organizations should monitor its progress and prepare, but should not treat these as current mandates.
What is current: healthcare chatbots must operate within HIPAA-eligible infrastructure. Business Associate Agreements with AI vendors need explicit coverage of AI-specific data handling — not just general PHI protection. A BAA that doesn't address how the vendor's AI model uses, stores, or trains on patient data is not an adequate safeguard.
PHI and PII must never flow into non-HIPAA-compliant AI platforms. This applies to third-party APIs, cloud services, and embedded AI features from vendors who have not executed a valid BAA.
State Laws That Layer on Top of Federal Rules
Federal rules set the floor — but three state laws impose additional restrictions that healthcare chatbot operators must account for:
| State | Law | Effective | Key Restriction |
|---|---|---|---|
| California | AB 489 | Jan. 1, 2026 | Prohibits AI from falsely implying care is from a licensed professional |
| Illinois | HB 1806 | Aug. 1, 2025 | Bans AI-generated therapy or treatment plans without licensed-professional review; up to $10,000 per violation |
| Texas | SB 815 | Sept. 1, 2025 | Prohibits automated adverse coverage determinations without human oversight |
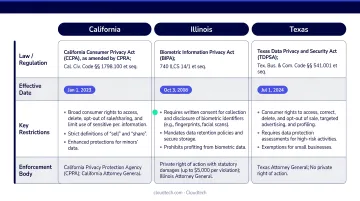
Healthcare chatbot operators need a compliance map that accounts for both federal requirements and the state laws applicable to their patient population. A chatbot deployed to patients in Illinois faces different legal constraints than one serving patients in states without comparable legislation.
Common Guardrail Mistakes to Avoid
Treating Guardrails as a Launch Checklist
A chatbot validated at deployment does not remain safe indefinitely. Clinical data patterns shift, patient language evolves, and model behavior drifts — a system that passes initial testing can degrade to unsafe performance without continuous monitoring to catch the change.
Post-deployment monitoring is not a nice-to-have. It's the mechanism that catches what pre-deployment testing missed and what real-world usage reveals over time.
Skipping Bias Testing Under Deadline Pressure
Organizations rushing to deploy frequently cut bias validation under time-to-launch pressure. The result is a system that works adequately for majority patient populations while producing inaccurate or inappropriate responses for underrepresented groups. The Tessa case illustrates what happens when scope drift goes undetected — but the bias testing gap creates a slower, less visible version of the same risk: a chatbot systematically underserving patients it was built to help.
Designing Escalation as a Last Resort
Many healthcare chatbot deployments treat human escalation as an edge-case fallback. Patients in distress end up cycling through automated responses before reaching a person. Configure escalation triggers to err on the side of transferring sooner. The cost of an unnecessary human handoff is far lower than the cost of a patient in crisis who couldn't get through.
Assuming Vendor AI Is Compliant by Default
That HIMSS finding carries real weight here: 42% of healthcare organizations lacked AI approval processes. Shadow AI risk extends directly to vendor-supplied tools — a third-party platform processing patient queries may handle PHI entirely outside your approved infrastructure.
Before any patient interaction goes live, verify:
- Vendor compliance status against your organization's approved AI processes
- Whether PHI flows through infrastructure covered by a signed BAA
- That the BAA includes explicit AI-specific clauses, not just general data handling terms
- Whether governance controls you assume are in place are actually contractually required
Conclusion
Safe healthcare chatbot deployment requires three disciplines working continuously together: pre-deployment validation that tests for real-world performance and bias, real-time guardrails that enforce clinical scope and escalation, and post-deployment monitoring that catches drift before patients are harmed. None of these phases can compensate for gaps in the others.
Organizations that treat these controls as infrastructure rather than compliance overhead end up with better patient outcomes and avoid the regulatory and reputational costs of guardrail failures.
Cloudtech helps healthcare organizations build HIPAA-compliant AI chatbot architectures on AWS that embed these principles from day one. As an AWS Advanced Tier Partner, Cloudtech delivers pre-packaged solutions in weeks — often with AWS Partner Funding that reduces out-of-pocket cost. If your organization is planning a healthcare chatbot deployment, connect with our team to scope the right guardrail architecture for your environment.
Frequently Asked Questions
What are some examples of AI guardrails?
Common examples include topic denial filters that block clinical advice requests, escalation triggers that route distressed patients to human agents, response supervision checks that catch hallucinated information, and bias detection checks that validate outputs across patient demographics. No single guardrail is sufficient — these controls work together.
What is the difference between AI guardrails and AI governance in healthcare?
Guardrails are the technical controls built into a chatbot — content filters, escalation logic, scope limits. Governance is the organizational framework (committees, policies, audit cycles) that decides which guardrails are required and keeps them effective. Guardrails without governance drift; governance without guardrails has nothing to enforce.
How do healthcare chatbots stay HIPAA compliant?
HIPAA compliance requires chatbots to operate within HIPAA-eligible infrastructure, avoid routing PHI to non-covered AI platforms, maintain audit logs of interactions, and execute AI-specific Business Associate Agreements with vendors. The proposed HIPAA Security Rule update would add stronger risk analysis requirements — healthcare organizations should monitor its finalization and prepare their AI systems accordingly.
When should a healthcare chatbot escalate to a human?
Key triggers include patient distress or crisis, requests for clinical advice, sensitive billing disputes, repeated session failures, and any explicit request for a human. Configure escalation to transfer sooner rather than later — the cost of an unnecessary handoff is low; missing a patient in crisis is not.
What happens if an AI healthcare chatbot gives wrong medical advice?
Incorrect clinical information can cause direct patient harm, expose the organization to HIPAA liability, and potentially trigger liability under other legal frameworks depending on the claim. This is why clinical scope guardrails and response supervision must prevent chatbots from generating medical recommendations in the first place — the safeguard has to exist upstream of the output, not as a correction after the fact.
How often should AI guardrails be tested and updated?
Continuous post-deployment monitoring is the baseline, with regression testing run after any model or workflow update. At minimum, a quarterly bias and performance audit catches the gradual drift that data distribution changes introduce — too slow for real-time alerts, but fast enough to degrade performance over months.