Introduction
Physicians today spend more time facing screens than facing patients. According to the AMA, office-based physicians log more than 5 EHR hours for every 8 hours scheduled with patients — and that burden follows them home. A 2024 JAMA Network Open analysis of over 10,000 family physicians found burnout rates near 42%, with after-hours EHR time directly linked to higher burnout odds.
Generative AI (GenAI) represents a different kind of fix than anything EHRs have tried before. Earlier AI flagged patterns and triggered alerts. GenAI creates — it drafts a clinical note from a conversation, summarizes a stack of records into a single paragraph, or composes a patient message response. That distinction is what makes it so relevant to EHR modernization.
This guide covers what GenAI actually does inside an EHR, the use cases gaining real traction, and the benefits and risks healthcare organizations must weigh. Whether you're a clinical informatics leader, a health IT director, or a smaller health system evaluating AI adoption, you'll leave with a clear-eyed view of what's ready to deploy, what's still maturing, and what infrastructure makes it all work.
Key Takeaways
- GenAI automates clinical documentation, summarizes patient records, and drafts patient communications directly inside EHR workflows
- Epic, Oracle, and eClinicalWorks are actively building GenAI capabilities into their platforms, with adoption accelerating
- GenAI cuts documentation burden and improves patient communication, but hallucinations and bias require active human oversight
- HIPAA-compliant cloud infrastructure — particularly on AWS — is the required foundation for any AI-powered EHR deployment
- Start with lower-risk use cases, build human review workflows first, then expand
What Generative AI Actually Does Inside an EHR
From Alerts to Outputs
Traditional EHR AI worked by detecting patterns — flagging a sepsis risk score, alerting on a missed medication dose, or surfacing a care gap. That's useful, but it's passive. GenAI goes further: it generates new content directly from clinical inputs.
Picture a primary care physician finishing a 20-minute visit. Instead of spending another 10 minutes writing a SOAP note, she opens the chart and finds a near-complete draft already structured — chief complaint, history, assessment, plan — pulled from the conversation that just happened. She reviews it, makes two edits, and signs off. That's ambient documentation powered by GenAI.
How It Works (Without the Jargon)
That physician scenario runs on large language models (LLMs) — AI systems trained on vast text datasets to predict the best next word, sentence, or summary for a given input. Under the hood, that's what GenAI tools inside EHRs are doing.
In clinical settings, those inputs include:
- Real-time transcripts from patient-clinician conversations
- Imaging findings and structured lab results
- Prior visit notes, referral documents, and care summaries
- Patient portal messages
The quality of outputs depends on two things: the quality of the underlying data, and how well the human review process is designed. Neither can be skipped.
Two examples show how this is rolling out in practice:
- Epic's HIPAA-compliant GenAI pipeline integrates GPT-4 for patient-response drafts, handoff summaries, and provider insights
- Oracle's Clinical AI Agent, announced in October 2024, is now live at health systems including AtlantiCare and Billings Clinic
Key Use Cases: How Generative AI Is Transforming EHR Workflows
Ambient Clinical Documentation
Ambient documentation is the fastest-growing GenAI application in healthcare. The workflow: a microphone captures the clinical encounter in real time, speech recognition converts audio to text, and an LLM structures that content into a note template — SOAP format, HPI, or whatever the EHR requires.
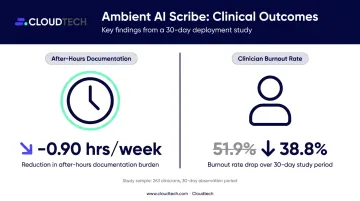
A multicenter quality-improvement study of 263 clinicians found that ambient AI scribes reduced after-hours documentation by 0.90 hours per week, with burnout dropping from 51.9% to 38.8% after 30 days. These are pre/post findings, not randomized results, but the direction is consistent across multiple health systems.
Emory Healthcare, Stanford Health Care, and Kaiser Permanente have all announced or deployed ambient documentation tools integrated with Epic. At this scale, ambient documentation has moved from experiment to standard consideration.
Clinical Record Summarization
Interoperability platforms like CommonWell and Health Gorilla now deliver dozens of clinical summary documents (CCDs) per patient encounter. Reading 30 documents before a visit isn't realistic. GenAI can synthesize CCDs, lab results, imaging reports, and prior notes into a single briefing a clinician can review in minutes.
The evidence is encouraging but still early. An EHR-integrated summarization study tested with emergency physicians found a 9.13% reduction in review time — from 2.11 to 1.92 minutes — though the difference was not statistically significant. Expect more definitive data as deployment scales beyond pilot cohorts.
AI-Assisted Patient Communication
Portal messages have doubled since 2020. A 2021 JAMIA study found that physicians spend an average of 52 minutes per workday on inbox work, with 37% occurring outside formal hours — the "pajama time" problem.
GenAI can draft portal message responses for clinician review before sending. A blinded comparison of 195 patient questions found evaluators preferred AI-generated responses 78.6% of the time — with empathy ratings of 45.1% for AI versus 4.6% for physicians. The study used Reddit posts rather than live portal messages, so production results may differ, but the quality signal is difficult to dismiss.
Diagnostic Report Generation with Vision-Language Models
Multimodal AI combines image recognition with language generation to draft radiology and pathology reports from imaging data. Microsoft's MAIRA-2 model generates grounded radiology reports from chest radiographs — currently a research system pending the clinical validation required for FDA clearance.
These tools are in early deployment and require rigorous clinician review at every output before findings reach the patient record.
Clinical Decision Support
GenAI integrated with EHR data can surface relevant clinical literature, flag drug interactions, or suggest differential diagnoses based on a patient's chart. In practice, this means:
- Surfacing guideline-concordant treatment options without a manual literature search
- Flagging contraindicated drug combinations before order entry
- Suggesting differential diagnoses when chart findings are ambiguous
FDA guidance requires that clinicians be able to independently review the basis of any qualifying recommendation, which sets a clear expectation for transparency in these tools.
Challenges and Risks That Cannot Be Ignored
AI Hallucinations in Clinical Settings
LLMs can generate confident, plausible-sounding content that is factually wrong. In a medical context, an invented lab value or fabricated drug interaction is a direct patient safety risk.
A 2025 primary-care summarization study found 1.47% hallucinations across nearly 13,000 annotated sentences, with 44% of those hallucinations rated as major. A separate 2024 study applying ChatGPT-4 to 54,729 ED notes found negation errors — the model misread "without helmet" as a positive finding.
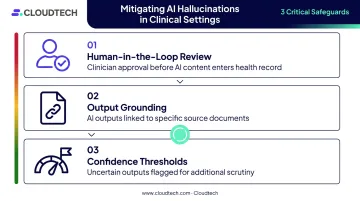
Mitigation approaches include:
- Human-in-the-loop review before any AI content enters the health record
- Grounding mechanisms that link AI outputs to specific source documents
- Confidence thresholds that flag uncertain outputs for additional scrutiny
Bias in AI-Generated Clinical Content
LLMs trained on historical healthcare data can perpetuate existing disparities. A 2023 study found that ChatGPT-3.5/4, Bard, and Claude all repeated false race-based claims about kidney function, lung capacity, and pain tolerance. These biases can be overt or embedded in language patterns.
Post-deployment monitoring is essential for catching bias drift before it reaches care decisions. Minimum safeguards include:
- Ongoing audits of AI outputs across patient demographic groups
- Feedback loops between clinicians and AI vendors when disparities surface
- Clear escalation paths when bias is detected in production
Legal Liability and Governance
Current consensus holds clinicians accountable for AI-assisted documentation they approve. But when a patient outcome is linked to an AI-generated note a clinician signed without full scrutiny, the liability boundaries get murky fast.
AMA's November 2024 policy requires physician consent and final review of AI-generated records. ONC's HTI-1 rule requires source-attribute transparency for predictive decision-support tools in certified health IT. Neither establishes a federal watermark mandate, but both signal the direction of travel.
Best practices for governance:
- Clearly mark which content was AI-generated versus human-authored
- Maintain audit trails of AI outputs and clinician modifications
- Establish vendor agreements requiring transparency about model changes
- Train clinical staff on AI limitations, not just AI features
Cloud Infrastructure: The Foundation AI-Powered EHRs Need
Running LLMs requires serious compute, low-latency data access, and on-demand scaling. Traditional on-premise EHR infrastructure wasn't built for any of those requirements. HIPAA-compliant cloud environments — particularly on AWS — provide the security, performance, and scalability that healthcare AI workloads demand.
AWS Services That Support AI-EHR Integration
AWS's HIPAA-eligible services directly applicable to AI-powered EHR architectures include:
| AWS Service | Role in AI-EHR Architecture |
|---|---|
| Amazon Bedrock | Managed LLM access for clinical summarization and generation |
| AWS HealthLake | FHIR R4-compliant storage and query for patient data |
| Amazon SageMaker | Model deployment and ML pipeline management |
| Amazon S3 | Scalable storage for large clinical datasets and documents |
| Amazon API Gateway | EHR integration layer connecting AI tools to existing systems |

AWS's reference architecture stores FHIR R4 data in HealthLake, retrieves patient histories through FHIR APIs, extracts attached documents with Amazon Textract, and routes combined context to Bedrock for patient-profile summarization. That's a practical starting point for most AI-EHR integration projects.
That architecture assumes a correctly configured environment, though. HIPAA eligibility on AWS isn't automatic — organizations still need a signed Business Associate Addendum and careful configuration before any PHI touches these services.
Making AI Infrastructure Accessible for Smaller Organizations
The most common concern from community hospitals and rural health clinics is cost. Enterprise-grade AI infrastructure sounds expensive — and it can be, if built from scratch without guidance.
Cloudtech, an AWS Advanced Tier Partner based in New York, has worked with healthcare organizations including Klamath Health Partnership to build HIPAA-compliant AWS data infrastructure — achieving 77% year-over-year infrastructure cost savings for one community health network.
Pre-built cloud accelerators and phased rollouts keep implementation within reach for smaller teams. AWS Partner Funding options can reduce upfront costs further for qualifying SMB health systems.
What's Next: The Future of AI-Enabled EHRs
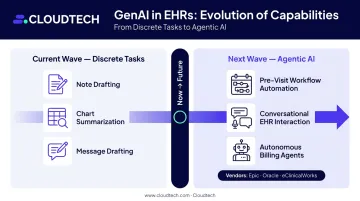
The current wave of GenAI in EHRs handles discrete tasks: draft a note, summarize a chart, compose a message. The next wave is agentic — multiple AI agents coordinating end-to-end workflows with minimal human handoffs at each step.
Epic is building agentic AI frameworks for pre-visit workflow preparation. Oracle announced conversational, contextual AI-driven EHR workflows in August 2025. eClinicalWorks demonstrated autonomous billing agents at HIMSS26. These are early announcements — not proven production deployments at scale — but the direction is unmistakable.
What this means for healthcare organizations planning AI adoption now:
- Establish AI use policies, clinician training programs, and performance monitoring now — governance built today positions organizations for agentic capabilities tomorrow.
- Invest in the cloud architecture that supports ambient documentation today; that same infrastructure will underpin multi-agent orchestration as it matures.
- Plan for evolving but persistent human oversight — even as AI automates more workflow steps, qualified clinician review remains a clinical, legal, and ethical requirement.
Organizations that start with solid infrastructure, clear governance, and lower-risk use cases won't just be ready for agentic AI — they'll already be running it while competitors are still evaluating.
Frequently Asked Questions
What is the difference between traditional AI and generative AI in EHR systems?
Traditional EHR AI detects patterns — flagging risk scores, triggering alerts, identifying care gaps. Generative AI creates new content: drafting clinical notes, summarizing records, composing patient messages. That shift from detection to generation is what makes GenAI so relevant to reducing documentation burden.
How does ambient documentation with generative AI work in an EHR?
Audio from the clinical encounter is captured in real time and converted to text via speech recognition. An LLM then structures that transcript into a clinical note template (SOAP, HPI, or another format), which the clinician reviews and approves before it enters the EHR.
Is generative AI safe to use in clinical EHR environments?
Real risks exist — hallucinations, negation errors, and demographic bias are documented in peer-reviewed research. With proper safeguards (human-in-the-loop review, output grounding, strong governance frameworks), GenAI can be deployed safely. Major health systems including Kaiser Permanente and Stanford are already doing it.
What are the biggest challenges healthcare organizations face when integrating generative AI into their EHR?
The three most common challenges are ensuring AI output accuracy and traceability, managing evolving compliance requirements, and maintaining cloud infrastructure capacity for AI workloads. Governance and infrastructure are typically underprepared relative to how quickly clinical tools have matured.
How does cloud infrastructure support AI-powered EHR modernization?
Cloud provides the scalable compute, HIPAA-compliant data storage, and low-latency processing that AI-powered EHR tools require. AWS services like Amazon Bedrock, HealthLake, and SageMaker can be deployed through managed solutions without building from scratch , reducing time to implementation and compliance risk.
Where should a healthcare organization start when adopting generative AI for its EHR?
Start with lower-risk, high-value use cases: ambient documentation, clinical record summarization, and patient message drafting. Establish human review workflows before expanding, and build on a secure, HIPAA-compliant cloud foundation before scaling further.