Introduction
Physicians are drowning in paperwork. According to a foundational study in the Annals of Internal Medicine, for every hour of direct patient care, clinicians spend nearly two additional hours on EHR documentation and desk work. At the same time, the American Medical Association reports physician burnout still affects 41.9% of doctors — even after three consecutive years of decline.
That documentation burden is exactly where generative AI differs from earlier clinical tools. Where previous AI systems classified or predicted, generative AI produces new content — clinical notes, synthetic training images, novel drug candidates — making it a direct match for healthcare's most stubborn bottlenecks.
This article covers what generative AI actually does in clinical settings, which applications have real evidence behind them, what risks demand governance before deployment, and how healthcare organizations can move from exploration to live production.
Key Takeaways:
- The generative AI healthcare market is projected to hit $48.23B by 2035, growing at 33.71% CAGR
- Start with clinical documentation — it's the most mature, lowest-risk deployment path
- No clinical deployment should go live without human-in-the-loop oversight in place
- HIPAA compliance is determined by infrastructure architecture, not the AI model itself
- AWS Bedrock, HealthLake, and HealthScribe are HIPAA-eligible services built for healthcare workloads
What Is Generative AI in Healthcare?
Traditional AI in healthcare classifies or predicts — flagging a lab value as abnormal, for instance, or scoring a readmission risk. Generative AI goes further: it produces new content from learned patterns. That distinction matters enormously for clinical workflows, because the most time-consuming tasks in medicine involve creation — writing notes, drafting authorization letters, designing drug molecules.
The Data Inputs That Drive These Models
Generative AI models are only as good as the data they train on. In healthcare, those inputs span nearly every type of clinical record:
- Electronic Health Records (EHRs) — structured clinical history, medications, diagnoses
- Medical imaging data — MRI, CT, X-ray, and ultrasound scans
- Genomic and multi-omics data for precision medicine and drug discovery
- Physician notes and transcripts — unstructured text that LLMs can parse and restructure
- Drug development records, including compound data and clinical trial outcomes
A model trained on incomplete or non-representative records will produce outputs that reflect those gaps — which in a clinical context can mean wrong dosage suggestions, missed diagnoses, or biased patient risk scores.
Three Technology Types Worth Knowing
| Technology | Primary Use in Healthcare |
|---|---|
| Large Language Models (LLMs) | Clinical documentation, patient chatbots, prior auth drafting |
| Vision-Language Models | Medical imaging analysis, radiology report generation |
| Generative Adversarial Networks (GANs) | Synthetic training data, image reconstruction and enhancement |
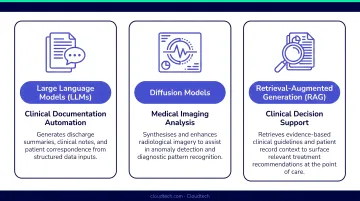
In practice, the most capable healthcare AI platforms layer all three — using an LLM to draft a radiology report while a vision model analyzes the underlying scan.
Key Applications of Generative AI in Healthcare
Clinical Documentation and Administrative Automation
This is where generative AI has the clearest operational track record. LLMs can listen to physician-patient conversations and automatically generate structured clinical notes, prior authorization requests, and insurance verification — without the clinician typing a word.
The numbers are concrete. Studies of ambient AI scribes report an average 7 minutes saved per patient encounter (Nuance DAX data), with documentation time per encounter dropping from 6.2 to 5.3 minutes in systems using Abridge. Across a full patient day, those minutes add up to hours.
Prior authorization automation is equally compelling. Deloitte data shows AI-enabled appeal-letter generation running up to 30x faster than manual drafting — freeing clinical staff from one of medicine's most frustrating administrative tasks.

Medical Imaging Enhancement
Generative models (particularly GANs and diffusion models ) improve MRI and CT scan quality by removing noise and reconstructing clearer images. They also generate synthetic training data to address the persistent scarcity of labeled medical images, which has historically slowed AI development in radiology.
Current evidence supports generative imaging AI for three primary use cases:
- Image augmentation — enhancing scan resolution and reducing noise artifacts
- Data reconstruction — filling gaps in incomplete imaging datasets with synthetic samples
- Workflow support — triaging scan queues and flagging anomalies for radiologist review
Claims of broad diagnostic superiority over radiologists aren't yet backed by consistent clinical validation. Human radiologist oversight remains essential.
Drug Discovery Acceleration
According to a 2024 GAO report (GAO-24-107634), approximately 70 generative AI-assisted drug candidates were in clinical trials as of December 2023. None had reached market at publication — the pipeline, however, signals where this is heading.
Generative models design novel molecular structures by simulating interactions with biological targets, running experiments computationally that would take years in a lab. McKinsey estimates this could create $60B–$110B in annual value for pharma and life sciences. For most small healthcare organizations, this remains a horizon-watch area rather than an active deployment priority.
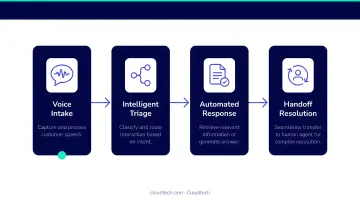
Patient-Facing AI Tools and Personalized Treatment
AI-powered virtual health assistants now handle patient interactions 24/7. Common capabilities include:
- Symptom triage — guiding patients through structured intake before a clinician reviews
- Appointment scheduling — booking and rescheduling without staff involvement
- Medication reminders — automated follow-ups to support adherence
- Care pathway guidance — directing patients to the right level of care
Research on AI chatbots in healthcare shows increased patient interactions by 30% and reduced consultation wait times by approximately 15%.
Personalized treatment planning takes this further, combining genomic data, lifestyle factors, and medical history to generate individualized therapy recommendations. Peer-reviewed precision medicine literature confirms multimodal AI — systems that combine text, imaging, and genomic data — can support targeted therapy selection. For most regional providers, though, this remains a research-stage capability rather than a live production tool.
Benefits for Healthcare Organizations
Reduced Clinician Burnout
The math is straightforward: if physicians spend nearly 2 hours on documentation for every 1 hour of patient care, automating documentation reclaims a significant share of the clinical day. A 2026 McKinsey survey found 54% of care providers have already deployed generative AI for clinical productivity — a number that would have been unthinkable three years ago.
Operational Efficiency and Cost Reduction
That productivity momentum extends to the bottom line. The same McKinsey survey found 82% of healthcare leaders expect positive generative AI ROI, with 45% quantifying expected returns at 2x–4x their investment. These are survey benchmarks, not audited financials — but the trend holds across multiple independent sources.
Key efficiency gains appear in:
- Claims processing and prior authorization turnaround
- Patient flow forecasting and staffing optimization
- Hospital resource allocation across departments
Research Acceleration
Synthetic data generated by AI models lets researchers run more experiments without exposing real patient records. For rare disease research — where real-world datasets are tiny — this is particularly valuable.
Key research benefits include:
- Compresses early-stage drug discovery from years to months using AI-generated molecular candidates
- Enables larger experiment volumes without privacy risk through synthetic patient data
- Accelerates rare disease research where real-world sample sizes are too small to be statistically useful
Challenges and Risks to Address
Hallucinations and Clinical Safety
Generative models can produce outputs that are fluent, confident, and wrong. In a clinical context — a mischaracterized drug interaction, an incorrect symptom summary — that's a patient safety risk. Peer-reviewed literature has explicitly flagged this, calling for evidence-based controls before any clinical deployment.
Human-in-the-loop validation for every clinical output is essential. FDA clinical decision support guidance reinforces this, noting that software falls outside device regulation only when a clinician can independently review the rationale behind recommendations.
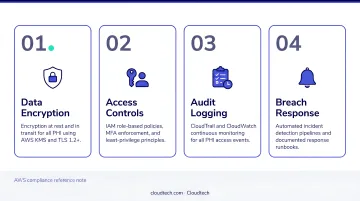
Data Privacy and HIPAA Compliance
Training AI models requires large volumes of sensitive patient data. IBM's 2025 Cost of a Data Breach Report found healthcare had the highest average breach cost of any sector at $7.42M — nearly double the global average.
HIPAA compliance architecture must address:
- De-identification via HHS-approved Expert Determination or Safe Harbor methods
- Business Associate Agreements (BAAs) with every vendor handling PHI
- Access controls limiting which users and systems can query patient data
- Prompt and transcript security — model inputs are PHI if they contain patient information
Algorithmic Bias and Integration Complexity
If training data underrepresents certain populations — by age, race, geography, or gender — the model will systematically underperform for those groups. A landmark Science study found that a widely used population-health algorithm reduced Black patients identified for extra care by more than half due to a biased proxy label.
Uneven data representation isn't the only structural barrier. Integration remains a persistent obstacle for most healthcare organizations, even as adoption grows. Common friction points include:
- Interoperability gaps — ONC data shows 70% of non-federal acute care hospitals participate in all four interoperability domains, but meaningful gaps remain
- Fragmented legacy systems that require significant data normalization before generative AI can work reliably across departments
- Inconsistent data formats across EHRs, billing systems, and care management platforms
Generative AI Healthcare Trends to Watch
Three converging shifts are reshaping how healthcare organizations approach generative AI right now — and each one has direct implications for how you build, deploy, and govern these systems.
- Multimodal AI models are moving beyond text-only LLMs. Newer systems simultaneously process imaging, genomics, vitals, and clinical notes — enabling richer clinical decision support than any single-modality tool can provide. WHO's AI ethics and governance guidance for large multimodal models means organizations need documented governance frameworks before deployment, not after.
- Synthetic data is an established technique for addressing data scarcity and privacy constraints. Radiology literature confirms that AI-generated synthetic imaging data can expand training sets without exposing patient identity — though generating realistic, de-identified data at scale remains technically demanding.
- Regulatory timelines are tightening. FDA released draft guidance on AI-enabled device software functions in January 2025. CMS has published human oversight requirements for AI-assisted care decisions. Organizations deploying generative AI now need audit-ready, explainable systems — not just functional ones.
How Healthcare Organizations Can Deploy Generative AI on AWS
Three prerequisites must be in place before any AI model goes live:
- A HIPAA-eligible cloud environment with a signed BAA and access controls configured before data flows in
- Clean, accessible data pipelines — EHR data, imaging, and clinical records normalized and queryable
- Clearly defined use cases with measurable success criteria — without specific clinical targets, even well-built models drift
AWS offers purpose-built services that compress deployment timelines:
- Amazon Bedrock — managed access to foundation models, HIPAA-eligible with proper BAA in place
- Amazon HealthLake — FHIR-compliant storage and analytics for structured health data
- AWS HealthScribe — combines speech recognition and generative AI to transcribe clinical conversations and generate documentation automatically

Those services create a strong foundation, but eligibility is not the same as compliance. Using HIPAA-eligible services is necessary — the architecture, data governance, and access controls also need validation before PHI touches any model.
Healthcare organizations that engage Cloudtech, an AWS Advanced Tier Partner with healthcare clients including Klamath Health Partnership, gain AWS-certified architects with HIPAA compliance experience designed into every deployment from day one. The team's structured discovery process starts with a one-day workshop to map infrastructure, compliance requirements, and clinical use cases before a single line of code is written.
That scoping discipline is what separates a successful pilot from a costly rebuild six months later.
Frequently Asked Questions
How can generative AI be used in healthcare?
The primary use cases span clinical documentation automation, medical imaging enhancement, drug discovery, patient-facing virtual assistants, and personalized treatment planning. Documentation automation has the strongest current evidence base and lowest deployment risk for most healthcare organizations.
What are the top generative AI model types used in healthcare?
Three categories dominate healthcare AI deployments:
- LLMs for clinical documentation and text-based tasks
- Vision-language models for imaging and radiology analysis
- Healthcare-specific LLMs trained on clinical data for terminology accuracy
Domain-specific models consistently outperform general-purpose models on clinical documentation tasks.
What are the biggest risks of generative AI in healthcare?
The top three risks are hallucinations producing clinically unsafe outputs, HIPAA data privacy violations, and algorithmic bias against underrepresented patient populations. Addressing these requires human oversight, governance frameworks, and regular bias auditing — none of which are optional in a regulated clinical environment.
Is generative AI in healthcare HIPAA compliant?
Generative AI is neither inherently compliant nor non-compliant. Compliance depends on infrastructure architecture, active BAAs with each vendor, and how PHI is secured across prompts, transcripts, and training data.
How long does it take to implement generative AI in a healthcare organization?
Focused deployments on pre-built platforms like AWS HealthScribe can go live in weeks. Enterprise-wide programs spanning multiple departments typically run several months to over a year, depending on infrastructure readiness and use case complexity.